Medication reference
Enzalutamide
Androgen Receptor Inhibitor [EPC] — ORAL
Enzalutamide — Androgen Receptor Inhibitor [EPC]. INDICATIONS AND USAGE XTANDI ® is indicated for the treatment of patients with: • castration-resistant prostate cancer (CRPC) • metastatic castration-
Brand names
Xtandi
Active ingredients
ENZALUTAMIDE
Indications
INDICATIONS AND USAGE XTANDI ® is indicated for the treatment of patients with: • castration-resistant prostate cancer (CRPC) • metastatic castration-sensitive prostate cancer (mCSPC) • non‑metastatic castration‑sensitive prostate cancer (nmCSPC) with biochemical recurrence at high risk for metastasis (high-risk BCR) XTANDI is an androgen receptor inhibitor indicated for the treatment of patients with: • castration-resistant prostate cancer. ( 1 ) • metastatic castration-sensitive prostate cancer. ( 1 ) • non‑metastatic castration‑sensitive prostate cancer with biochemical recurrence at high risk for metastasis. ( 1 )
Dosage
DOSAGE AND ADMINISTRATION • Take XTANDI 160 mg administered orally once daily with or without food. ( 2.1 ) • Advise patients to take each capsule or tablet whole with a sufficient amount of water to ensure that all medication is successfully swallowed. ( 2.1 , 5.7 ) • Patients receiving XTANDI for castration-resistant prostate cancer, or metastatic castration sensitive prostate cancer should also receive a gonadotropin-releasing hormone (GnRH) analog concurrently or should have had bilateral orchiectomy. ( 2.1 ) • Patients with non-metastatic castration-sensitive prostate cancer with biochemical recurrence at high risk for metastasis may be treated with or without a GnRH analog. ( 2.1 ) 2.1 Recommended Dosage The recommended dosage of XTANDI is 160 mg administered orally once daily with or without food [see Clinical Pharmacology ( 12.3 )] until disease progression or unacceptable toxicity. Advise patients to take each capsule or tablet whole with a sufficient amount of water to ensure that all medication is successfully swallowed. Do NOT chew, dissolve, or open the capsules. Do NOT cut, crush, or chew the tablets. Patients with CRPC or mCSPC receiving XTANDI should also receive a gonadotropic-releasing hormone (GnRH) analog concurrently or should have had bilateral orchiectomy. Patients with nmCSPC with high-risk BCR may be treated with XTANDI with or without a GnRH analog. For patients who receive XTANDI with or without a GnRH analog, treatment can be suspended if PSA is undetectable (< 0.2 ng/mL) after 36 weeks of therapy. Reinitiate treatment when PSA has increased to ≥ 2.0 ng/mL for patients who had prior radical prostatectomy or ≥ 5.0 ng/mL for patients who had prior primary radiation therapy [see Clinical Studies ( 14 )] . 2.2 Dosage Modifications for Adverse Reactions If a patient experiences a ≥ Grade 3 or an intolerable adverse reaction, withhold XTANDI for one week or until symptoms improve to ≤ Grade 2, then resume at the same or a reduced dose (120 mg or 80 mg) if warranted [see Warnings and Precautions ( 5.1 , 5.2 )] . 2.3 Dosage Modifications for Drug Interactions Strong CYP2C8 Inhibitors Avoid the coadministration of strong CYP2C8 inhibitors. If the coadministration of a strong CYP2C8 inhibitor cannot be avoided, reduce the XTANDI dosage to 80 mg once daily. If the coadministration of the strong inhibitor is discontinued, increase the XTANDI dosage to the dosage used prior to initiation of the strong CYP2C8 inhibitor [see Clinical Pharmacology ( 12.3 )]. Strong CYP3A4 Inducers Avoid the coadministration of strong CYP3A4 inducers. If the coadministration of a strong CYP3A4 inducer cannot be avoided, increase the XTANDI dosage from 160 mg to 240 mg orally once daily. If the coadministration of the strong CYP3A4 inducer is discontinued, decrease the XTANDI dosage to the dosage used prior to initiation of the strong CYP3A4 inducer [see Clinical Pharmacology ( 12.3 )].
Warnings
WARNINGS AND PRECAUTIONS • Seizure occurred in 0.6% of patients receiving XTANDI. In patients with predisposing factors, seizures were reported in 2.2% of patients. Permanently discontinue XTANDI in patients who develop a seizure during treatment. ( 5.1 ) • Posterior reversible encephalopathy syndrome (PRES): Discontinue XTANDI. ( 5.2 ) • Hypersensitivity: Discontinue XTANDI. ( 5.3 ) • Ischemic Heart Disease: Optimize management of cardiovascular risk factors. Discontinue XTANDI for Grade 3-4 adverse reactions ( 5.4 ) • Falls and Fractures: Evaluate patients for fracture and fall risk, and treat patients with bone-targeted agents according to established guidelines. ( 5.5 ) • Embryo-Fetal Toxicity: XTANDI can cause fetal harm and loss of pregnancy. Advise males with female partners of reproductive potential to use effective contraception. ( 5.6 , 8.1 , 8.3 ) • Severe Dysphagia or Choking Related to Product Size: Consider using smaller XTANDI tablet(s) in patients who have difficulty swallowing. Discontinue XTANDI for patients who cannot swallow capsules or tablets. ( 2.1 , 5.7 ) • Interference with Immunoassay Measurement of Digoxin XTANDI can interfere with certain digoxin immunoassays, resulting in falsely elevated digoxin plasma concentration results. ( 5.8 , 7.3 ) 5.1 Seizure Seizure occurred in 0.6% of patients receiving XTANDI in eight randomized clinical trials. In these trials, patients with predisposing factors for seizure were generally excluded. Seizure occurred from 13 to 2250 days after initiation of XTANDI. Patients experiencing seizure were permanently discontinued from therapy, and all seizure events resolved. In a single-arm trial designed to assess the risk of seizure in patients with pre-disposing factors for seizure, 8 of 366 (2.2%) XTANDI-treated patients experienced a seizure. Three of the 8 patients experienced a second seizure during continued treatment with XTANDI after their first seizure resolved. It is unknown whether anti-epileptic medications will prevent seizures with XTANDI. Patients in the study had one or more of the following pre-disposing factors: the use of medications that may lower the seizure threshold (~ 54%), history of traumatic brain or head injury (~ 28%), history of cerebrovascular accident or transient ischemic attack (~ 24%), and Alzheimer’s disease, meningioma, or leptomeningeal disease from prostate cancer, unexplained loss of consciousness within the last 12 months, past history of seizure, presence of a space occupying lesion of the brain, history of arteriovenous malformation, or history of brain infection (all < 5%). Approximately 17% of patients had more than one risk factor. Advise patients of the risk of developing a seizure while receiving XTANDI and of engaging in any activity where sudden loss of consciousness could cause serious harm to themselves or others. Permanently discontinue XTANDI in patients who develop a seizure during treatment. 5.2 Posterior Reversible Encephalopathy Syndrome (PRES) There have been reports of posterior reversible encephalopathy syndrome (PRES) in patients receiving XTANDI [see Adverse Reactions ( 6.2 )] . PRES is a neurological disorder which can present with rapidly evolving symptoms including seizure, headache, lethargy, confusion, blindness, and other visual and neurological disturbances, with or without associated hypertension. A diagnosis of PRES requires confirmation by brain imaging, preferably magnetic resonance imaging (MRI). Discontinue XTANDI in patients who develop PRES. 5.3 Hypersensitivity Hypersensitivity reactions, including edema of the face (0.5%), tongue (0.1%), or lip (0.1%) have been observed with enzalutamide in eight randomized clinical trials. Pharyngeal edema has been reported in post-marketing cases. Advise patients who experience any symptoms of hypersensitivity to temporarily discontinue XTANDI and promptly seek medical care. Permanently discontinue XTANDI for serious hypersensitivity reactions. 5.4 Ischemic Heart Disease In the combined data of five randomized, placebo-controlled clinical studies, ischemic heart disease occurred more commonly in patients on the XTANDI arm compared to patients on the placebo arm (3.5% vs 2%). Grade 3-4 ischemic events occurred in 1.8% of patients on the XTANDI arm compared to 1.1% on the placebo arm. Ischemic events led to death in 0.4% of patients on the XTANDI arm compared to 0.1% on the placebo arm. Monitor for signs and symptoms of ischemic heart disease. Optimize management of cardiovascular risk factors, such as hypertension, diabetes, or dyslipidemia. Discontinue XTANDI for Grade 3-4 ischemic heart disease. 5.5 Falls and Fractures Falls and fractures occurred in patients receiving XTANDI. Evaluate patients for fracture and fall risk. Monitor and manage patients at risk for fractures according to established treatment guidelines and consider use of bone-targeted agents. In the combined data of five randomized, placebo-controlled clinical studies, falls occurred in 12% of patients treated with XTANDI compared to 6% of patients treated with placebo. Falls were not associated with loss of consciousness or seizure. Fractures occurred in 13% of patients treated with XTANDI and in 6% of patients treated with placebo. Grade 3-4 fractures occurred in 3.4% of patients treated with XTANDI and in 1.9% of patients treated with placebo. The median time to onset of fracture was 420 days (range: 1 to 2348 days) for patients treated with XTANDI. Routine bone density assessment and treatment of osteoporosis with bone-targeted agents were not performed in the studies. 5.6 Embryo-Fetal Toxicity The safety and efficacy of XTANDI have not been established in females. Based on animal reproductive studies and mechanism of action, XTANDI can cause fetal harm and loss of pregnancy when administered to a pregnant female. Advise males with female partners of reproductive potential to use effective contraception during treatment with XTANDI and for 3 months after the last dose of XTANDI [see Use in Specific Populations ( 8.1 , 8.3 )] . 5.7 Dysphagia or Choking Severe dysphagia or choking, including events that could be life-threatening requiring medical intervention or fatal, can occur due to XTANDI product size. Advise patients to take each capsule or tablet whole with a sufficient amount of water to ensure that all medication is successfully swallowed. Consider use of a smaller tablet size of XTANDI in patients who have difficulty swallowing. Discontinue XTANDI for patients who cannot swallow capsules or tablets. 5.8 Interference with Immunoassay Measurement of Digoxin: XTANDI can interfere with certain digoxin immunoassays (e.g., Chemiluminescent Microparticle Immunoassays), resulting in falsely elevated digoxin plasma concentration results. Notify the laboratory conducting the digoxin plasma concentration assay to use an appropriate method in patients receiving XTANDI and digoxin [ see Drug Interactions ( 7.3 )] .
Contraindications
CONTRAINDICATIONS None. None. ( 4 )
Drug interactions
DRUG INTERACTIONS • Strong CYP2C8 Inhibitors: Avoid strong CYP2C8 inhibitors. If coadministration cannot be avoided, reduce the dosage of XTANDI. ( 2.3 , 7.1 ) • Strong CYP3A4 Inducers: Avoid strong CYP3A4 inducers. If coadministration cannot be avoided, increase the dosage of XTANDI. ( 2.3 , 7.1 ) • Avoid coadministration with certain CYP3A4, CYP2C9, or CYP2C19 substrates for which a minimal decrease in concentration may lead to therapeutic failure of the substrate. In cases where active metabolites are formed, there may be increased exposure to the active metabolites. ( 7.2 ) 7.1 Effect of Other Drugs on XTANDI Strong CYP2C8 Inhibitors The coadministration of XTANDI with gemfibrozil (a strong CYP2C8 inhibitor) increases plasma concentrations of enzalutamide plus N-desmethyl enzalutamide, which may increase the incidence and severity of adverse reactions of XTANDI. Avoid the coadministration of XTANDI with strong CYP2C8 inhibitors. If the coadministration of XTANDI with a strong CYP2C8 inhibitor cannot be avoided, reduce the dosage of XTANDI [see Dosage and Administration ( 2.3 ), Clinical Pharmacology ( 12.3 )]. Strong CYP3A4 Inducers The coadministration of XTANDI with rifampin (a strong CYP3A4 inducer and a moderate CYP2C8 inducer) decreases plasma concentrations of enzalutamide plus N-desmethyl enzalutamide, which may decrease the efficacy of XTANDI. Avoid the coadministration of XTANDI with strong CYP3A4 inducers. If the coadministration of XTANDI with a strong CYP3A4 inducer cannot be avoided, increase the dosage of XTANDI [see Dosage and Administration ( 2.3 ), Clinical Pharmacology ( 12.3 )]. 7.2 Effect of XTANDI on Other Drugs Certain CYP3A4, CYP2C9, or CYP2C19 Substrates XTANDI is a strong CYP3A4 inducer and a moderate CYP2C9 and CYP2C19 inducer. The coadministration of XTANDI decreases the concentrations of certain CYP3A4, CYP2C9, or CYP2C19 substrates [see Clinical Pharmacology ( 12.3 )] , which may reduce the efficacy of these substrates. Avoid the coadministration of XTANDI with certain CYP3A4, CYP2C9, or CYP2C19 substrates for which a minimal decrease in concentration may lead to therapeutic failure of the substrate. If the coadministration cannot be avoided, increase the dosage of these substrates in accordance with their Prescribing Information. In cases where active metabolites are formed, there may be increased exposure to the active metabolites. 7.3 Laboratory Test Interference XTANDI can interfere with certain digoxin immunoassays (e.g., Chemiluminescent Microparticle Immunoassays), resulting in falsely elevated digoxin plasma concentration results. Notify the laboratory conducting the digoxin plasma concentration assay to use an appropriate method in patients receiving XTANDI and digoxin [see Warnings and Precautions ( 5.8 )] .
Adverse reactions
ADVERSE REACTIONS The following is discussed in more detail in other sections of the labeling: • Seizure [see Warnings and Precautions ( 5.1 )] • Posterior Reversible Encephalopathy Syndrome (PRES) [see Warnings and Precautions ( 5.2 )] • Hypersensitivity [see Warnings and Precautions ( 5.3 )] • Ischemic Heart Disease [see Warnings and Precautions ( 5.4 )] • Falls and Fractures [see Warnings and Precautions ( 5.5 )] • Dysphagia or Choking [see Warnings and Precautions ( 5.7 )] The most common adverse reactions (≥ 10%) that occurred more frequently (≥ 2% over placebo) in the XTANDI-treated patients are musculoskeletal pain, fatigue, hot flush, constipation, decreased appetite, diarrhea, hypertension, hemorrhage, fall, fracture, and headache. ( 6.1 ) To report SUSPECTED ADVERSE REACTIONS, contact Astellas Pharma US, Inc. at 1-800-727-7003 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch . 6.1 Clinical Trial Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. The data in WARNINGS and PRECAUTIONS reflect eight randomized, controlled trials [AFFIRM, PREVAIL, TERRAIN, PROSPER, ARCHES, EMBARK, Asian PREVAIL (NCT02294461), and STRIVE (NCT01664923)] that were pooled to conduct safety analyses in patients with CRPC (N = 3651), mCSPC (N = 752), or nmCSPC with high‑risk BCR (N = 707) treated with XTANDI. Patients received XTANDI 160 mg (N = 5110) or placebo orally once daily (N = 2829) or bicalutamide 50 mg orally once daily (N = 387). In these eight trials, the median duration of treatment was 22.1 months (range: < 0.1 to 95.0) in patients that received XTANDI. In five placebo-controlled trials (AFFIRM, PROSPER, PREVAIL, ARCHES, and EMBARK), the median duration of treatment was 19.4 months (range: < 0.1 to 90.4) in the XTANDI group [see Clinical Studies ( 14 )]. In these five trials, the most common adverse reactions (≥ 10%) that occurred more frequently (≥ 2% over placebo) in the XTANDI-treated patients were musculoskeletal pain, fatigue, hot flush, constipation, decreased appetite, diarrhea, hypertension, hemorrhage, fall, fracture and headache. AFFIRM: XTANDI versus Placebo in Metastatic CRPC Following Chemotherapy AFFIRM enrolled 1199 patients with metastatic CRPC who had previously received docetaxel. The median duration of treatment was 8.3 months with XTANDI and 3.0 months with placebo. During the trial, 48% of patients on the XTANDI arm and 46% of patients on the placebo arm received glucocorticoids. Grade 3 and higher adverse reactions were reported among 47% of XTANDI-treated patients. Discontinuations due to adverse reactions were reported for 16% of XTANDI-treated patients. The most common adverse reaction leading to treatment discontinuation was seizure, which occurred in 0.9% of the XTANDI-treated patients compared to none (0%) of the placebo-treated patients. Table 1 shows adverse reactions reported in AFFIRM that occurred at a ≥ 2% higher frequency in the XTANDI arm compared to the placebo arm. Table 1. Adverse Reactions in AFFIRM XTANDI (N = 800) Placebo (N = 399) Grade 1-4 CTCAE v 4. (%) Grade 3-4 (%) Grade 1-4 (%) Grade 3-4 (%) General Disorders Asthenic Conditions Includes asthenia and fatigue. 51 9 44 9 Peripheral Edema 15 1 13 0.8 Musculoskeletal and Connective Tissue Disorders Back Pain 26 5 24 4 Arthralgia 21 2.5 17 1.8 Musculoskeletal Pain 15 1.3 12 0.3 Muscular Weakness 10 1.5 7 1.8 Musculoskeletal Stiffness 2.6 0.3 0.3 0 Gastrointestinal Disorders Diarrhea 22 1.1 18 0.3 Vascular Disorders Hot Flush 20 0 10 0 Hypertension 6 2.1 2.8 1.3 Nervous System Disorders Headache 12 0.9 5 0 Dizziness Includes dizziness and vertigo. 9 0.5 7 0.5 Spinal Cord Compression and Cauda Equina Syndrome 7 7 4.5 3.8 Paresthesia 7 0 4.5 0 Mental Impairment Disorders Includes amnesia, memory impairment, cognitive disorder, and disturbance in attention. 4.3 0.3 1.8 0 Hypoesthesia 4 0.3 1.8 0 Infections and Infestations Upper Respiratory Tract Infection Includes nasopharyngitis, upper respiratory tract infection, sinusitis, rhinitis, pharyngitis, and laryngitis. 11 0 6 0.3 Lower Respiratory Tract And Lung Infection Includes pneumonia, lower respiratory tract infection, bronchitis, and lung infection. 8 2.4 4.8 1.3 Psychiatric Disorders Insomnia 9 0 6 0.5 Anxiety 6 0.3 4 0 Renal and Urinary Disorders Hematuria 7 1.8 4.5 1 Pollakiuria 4.8 0 2.5 0 Injury, Poisoning and Procedural Complications Fall 4.6 0.3 1.3 0 Non-pathologic Fractures 4 1.4 0.8 0.3 Skin and Subcutaneous Tissue Disorders Pruritus 3.8 0 1.3 0 Dry Skin 3.5 0 1.3 0 Respiratory Disorders Epistaxis 3.3 0.1 1.3 0.3 PREVAIL: XTANDI versus Placebo in Chemotherapy-naïve Metastatic CRPC PREVAIL enrolled 1717 patients with metastatic CRPC who had not received prior cytotoxic chemotherapy, of whom 1715 received at least one dose of study drug. The median duration of treatment was 17.5 months with XTANDI and 4.6 months with placebo. Grade 3-4 adverse reactions were reported in 44% of XTANDI-treated patients and 37% of placebo-treated patients. Discontinuations due to adverse reactions were reported for 6% of XTANDI-treated patients. The most common adverse reaction leading to treatment discontinuation was fatigue/asthenia, which occurred in 1% of patients on each treatment arm. Table 2 includes adverse reactions reported in PREVAIL that occurred at a ≥ 2% higher frequency in the XTANDI arm compared to the placebo arm. Table 2. Adverse Reactions in PREVAIL XTANDI (N = 871) Placebo (N = 844) Grade 1-4 CTCAE v 4. (%) Grade 3-4 (%) Grade 1-4 (%) Grade 3-4 (%) General Disorders Asthenic Conditions Includes asthenia and fatigue. 47 3.4 33 2.8 Peripheral Edema 12 0.2 8 0.4 Musculoskeletal and Connective Tissue Disorders Back Pain 29 2 22 3 Arthralgia 21 1.6 16 1.1 Gastrointestinal Disorders Constipation 23 0.7 17 0.4 Diarrhea 17 0.3 14 0.4 Vascular Disorders Hot Flush 18 0.1 8 0 Hypertension 14 7 4.1 2.3 Nervous System Disorders Dizziness Includes dizziness and vertigo. 11 0.3 7 0 Headache 11 0.2 7 0.4 Dysgeusia 8 0.1 3.7 0 Mental Impairment Disorders Includes amnesia, memory impairment, cognitive disorder, and disturbance in attention. 6 0 1.3 0.1 Restless Legs Syndrome 2.1 0.1 0.4 0 Respiratory Disorders Dyspnea Includes dyspnea, exertional dyspnea, and dyspnea at rest. 11 0.6 8 0.6 Infections and Infestations Upper Respiratory Tract Infection Includes nasopharyngitis, upper respiratory tract infection, sinusitis, rhinitis, pharyngitis, and laryngitis. 16 0 11 0 Lower Respiratory Tract And Lung Infection Includes pneumonia, lower respiratory tract infection, bronchitis, and lung infection. 8 1.5 4.7 1.1 Psychiatric Disorders Insomnia 8 0.1 6 0 Renal and Urinary Disorders Hematuria 9 1.3 6 1.3 Injury, Poisoning and Procedural Complications Fall 13 1.6 5 0.7 Non-Pathological Fracture 9 2.1 3 1.1 Metabolism and Nutrition Disorders Decreased Appetite 19 0.3 16 0.7 Investigations Weight Decreased 12 0.8 8 0.2 Reproductive System and Breast Disorders Gynecomastia 3.4 0 1.4 0 TERRAIN: XTANDI versus Bicalutamide in Chemotherapy-naïve Metastatic CRPC TERRAIN enrolled 375 patients with metastatic CRPC who had not received prior cytotoxic chemotherapy, of whom 372 received at least one dose of study drug. The median duration of treatment was 11.6 months with XTANDI and 5.8 months with bicalutamide. Discontinuations with an adverse reaction as the primary reason were reported for 8% of XTANDI-treated patients and 6% of bicalutamide-treated patients. The most common adverse reactions leading to treatment discontinuation were back pain and pathological fracture, which occurred in 3.8% of XTANDI-treated patients for each event and in 2.1% and 1.6% of bicalutamide-treated patients, respectively. Table 3 shows overall and common adverse reactions (≥ 10%) in XTANDI-treated patients. Table 3. Adverse Reactions in
Mechanism of action
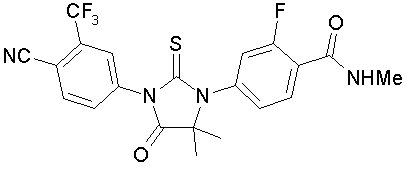
Mechanism of Action Enzalutamide is an androgen receptor inhibitor that acts on different steps in the androgen receptor signaling pathway. Enzalutamide has been shown to competitively inhibit androgen binding to androgen receptors; and consequently, inhibits nuclear translocation of androgen receptors and their interaction with DNA. A major metabolite, N‑desmethyl enzalutamide, exhibited similar in vitro activity to enzalutamide. Enzalutamide decreased proliferation and induced cell death of prostate cancer cells in vitro , and decreased tumor volume in a mouse prostate cancer xenograft model.
Available forms (6)
NDC examples
0469-01250469-06250469-0725
Indicated ICD-10 codes
Treats these conditions
Source: openFDA + RxNorm · 2026
Look up another medication