Linaclotide — Guanylate Cyclase-C Agonist [EPC]. INDICATIONS AND USAGE LINZESS is indicated for the treatment of: • irritable bowel syndrome with constipation (IBS-C) in adults and pediatric patients
Boxed warning
WARNING: RISK OF SERIOUS DEHYDRATION IN PEDIATRIC PATIENTS LESS THAN 2 YEARS OF AGE LINZESS is contraindicated in patients less than 2 years of age; in nonclinical studies in neonatal mice, administration of a single, clinically relevant adult oral dose of linaclotide caused deaths due to dehydration [see Contraindications ( 4 ), Warnings and Precautions ( 5.1 ), Use in Specific Populations ( 8.4 )]. WARNING: RISK OF SERIOUS DEHYDRATION IN PEDIATRIC PATIENTS LESS THAN 2 YEARS OF AGE See full prescribing information for complete boxed warning. LINZESS is contraindicated in patients less than 2 years of age; in neonatal mice, linaclotide caused deaths due to dehydration. ( 4 , 5.1 , 8.4 )
INDICATIONS AND USAGE LINZESS is indicated for the treatment of: • irritable bowel syndrome with constipation (IBS-C) in adults and pediatric patients 7 years of age and older • chronic idiopathic constipation (CIC) in adults • functional constipation (FC) in pediatric patients 2 years of age and older LINZESS is a guanylate cyclase-C agonist indicated for treatment of: Irritable bowel syndrome with constipation (IBS-C) in adults and pediatric patients 7 years of age and older. ( 1 ) Chronic idiopathic constipation (CIC) in adults. ( 1 ) Functional constipation (FC) in pediatric patients 2 years of age and older. ( 1 )
Dosage
DOSAGE AND ADMINISTRATION The recommended dosage in adults is: IBS-C : 290 mcg orally once daily. ( 2.1 ) CIC : 145 mcg orally once daily or 72 mcg orally once daily based on individual presentation or tolerability. ( 2.1 ) The recommended dosage in pediatric patients: 7 years of age and older with IBS-C : 145 mcg orally once daily. ( 2.1 ) 2 years of age and older with FC : 72 mcg orally once daily. ( 2.1 ) Administration Instructions ( 2.2 ): Take on empty stomach at least 30 minutes prior to a meal at approximately the same time each day. Do not crush or chew LINZESS capsule or capsule contents. For patients who have difficulty swallowing capsules whole or those with a nasogastric or gastrostomy tube, see full prescribing information for instructions for opening the capsule and administering with applesauce or water. 2.1 Recommended Dosage Irritable Bowel Syndrome with Constipation (IBS-C) : The recommended dosage of LINZESS is: • Adults : 290 mcg orally once daily • Pediatric patients 7 years of age and older : 145 mcg orally once daily Chronic Idiopathic Constipation (CIC) in Adults The recommended dosage of LINZESS in adults is 145 mcg orally once daily. A dosage of 72 mcg once daily may be used based on individual presentation or tolerability. Functional Constipation (FC) in Pediatric Patients 2 Years of Age and Older The recommended dosage of LINZESS in pediatric patients 2 years of age and older is 72 mcg orally once daily. 2.2 Preparation and Administration Instructions • Take LINZESS on an empty stomach, at least 30 minutes prior to a meal at approximately the same time each day. • If a dose is missed, skip the missed dose and take the next dose at the regular time. Do not take 2 doses at the same time. • Do not crush or chew LINZESS capsule or capsule contents. • Swallow LINZESS capsule whole. • For patients who are unable to swallow the capsule whole, LINZESS capsules can be opened and administered orally in either applesauce or with water or administered with water via a nasogastric or gastrostomy tube. Sprinkling of LINZESS beads on other soft foods or in other liquids has not been tested. Oral Administration in Applesauce Place one teaspoonful of room-temperature applesauce into a clean container. Open the capsule. Sprinkle the entire contents (beads) on applesauce. Consume the entire contents immediately. Do not chew the beads. Do not store the bead-applesauce mixture for later use. Oral Administration in Water Pour approximately 30 mL of room-temperature bottled water into a clean cup. Open the capsule. Sprinkle the entire contents (beads) into the water. Gently swirl beads and water for at least 20 seconds. Swallow the entire mixture of beads and water immediately. Add another 30 mL of water to any beads remaining in cup, swirl for 20 seconds, and swallow immediately. Do not store the bead-water mixture for later use. Note: The drug is coated on the surface of the beads and will dissolve off the beads into the water. The beads will remain visible and will not dissolve. Therefore, it is not necessary to consume all the beads to deliver the complete dose. Administration with Water via a Nasogastric or Gastrostomy Tube Open the capsule and empty the beads into a clean container with 30 mL of room-temperature bottled water. Mix by gently swirling beads for at least 20 seconds. Draw-up the beads and water mixture into an appropriately sized catheter-tipped syringe and apply rapid and steady pressure (10 mL/10 seconds) to dispense the syringe contents into the tube. Add another 30 mL of water to any beads remaining in the container and repeat the process. After administering the bead-water mixture, flush nasogastric/ gastrostomy tube with a minimum of 10 mL of water. Note: It is not necessary to flush all the beads through to deliver the complete dose.
Warnings
WARNINGS AND PRECAUTIONS Diarrhea: Patients may experience severe diarrhea. If severe diarrhea occurs, suspend dosing and rehydrate the patient. ( 5.2 ) 5.1 Risk of Serious Dehydration in Pediatric Patients Less Than 2 Years of Age LINZESS is contraindicated in patients less than 2 years of age. In neonatal mice (human age equivalent of approximately 0 to 28 days), linaclotide increased fluid secretion as a consequence of age-dependent elevated GC-C agonism which was associated with increased mortality within the first 24 hours due to dehydration. There was no age-dependent trend in GC-C intestinal expression in a clinical study of children 2 to less than 18 years of age; however, there are insufficient data available on GC-C intestinal expression in children less than 2 years of age to assess the risk of developing diarrhea and its potentially serious consequences in these patients [see Warnings and Precautions ( 5.2 ) and Use in Specific Populations ( 8.4 ) ] . 5. 2 Diarrhea In adults, diarrhea was the most common adverse reaction of LINZESS-treated patients in the pooled IBS-C and CIC double-blind placebo-controlled trials. The incidence of diarrhea was similar between the IBS-C and CIC populations. Severe diarrhea was reported in 2% of adult patients with IBS-C or CIC treated with LINZESS 145 mcg or 290 mcg once daily, and in <1% of adult patients with CIC treated with LINZESS 72 mcg once daily [see Adverse Reactions ( 6.1 )] . In pediatric patients, diarrhea was also the most common adverse reaction in clinical trials of patients 7 to 17 years of age with IBS-C and 6 to 17 years of age with FC treated with LINZESS [see Adverse Reactions ( 6.1 )]. • In a double-blind trial of patients 7 to 17 years of age with IBS-C, diarrhea was reported in 7% and 8% of patients treated with LINZESS 145 mcg and 290 mcg once daily, respectively. One severe case of diarrhea was reported in the IBS-C trial at a dosage higher than the recommended LINZESS 145 mcg once daily dosage for IBS-C. • In a double-blind trial of patients 6 to 17 years of age with FC treated with LINZESS 72 mcg once daily, diarrhea was reported in 4% of patients, and one case of severe diarrhea was reported. In post-marketing experience, severe diarrhea associated with dizziness, syncope, hypotension and electrolyte abnormalities (hypokalemia and hyponatremia) requiring hospitalization or intravenous fluid administration have been reported in patients treated with LINZESS. If severe diarrhea occurs, suspend dosing and rehydrate the patient.
Contraindications
CONTRAINDICATIONS LINZESS is contraindicated in: Patients less than 2 years of age due to the risk of serious dehydration [see Warnings and Precautions ( 5.1 ), Use in Specific Populations ( 8.4 )] . Patients with known or suspected mechanical gastrointestinal obstruction. Patients less than 2 years of age. ( 4 , 5.1 , 8.4 ) Patients with known or suspected mechanical gastrointestinal obstruction. ( 4 )
Adverse reactions
ADVERSE REACTIONS Most common adverse reactions (≥2%) reported in adult patients with IBS-C or CIC are: diarrhea, abdominal pain, flatulence and abdominal distension. ( 6.1 ) Most common adverse reaction (≥2%) reported in pediatric patients 7 to 17 years of age with IBS-C and 6 to 17 years of age with FC is diarrhea. ( 6.1 ) To report SUSPECTED ADVERSE REACTIONS, contact AbbVie, Inc. at 1-800-633-9110 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. 6.1 Clinical Trials Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared with rates in the clinical trials of another drug and may not reflect the rates observed in practice. Demographic characteristics were comparable between treatment groups in all studies [see Clinical Studies ( 14.1 , 14.2 , 14.3 , 14.4 , 14.5 )] . Irritable Bowel Syndrome with Constipation (IBS-C) in Adults Most Common Adverse Reactions The data described below reflect exposure to LINZESS in the two placebo-controlled clinical trials involving 1605 adult patients with IBS-C (Trials 1 and 2) [see Clinical Studies ( 14.1 )] . Patients were randomized to receive placebo or 290 mcg LINZESS once daily on an empty stomach for up to 26 weeks. Table 1 provides the incidence of adverse reactions reported in at least 2% of IBS-C patients in the LINZESS treatment group and at an incidence that was greater than in the placebo group. Table 1: Most Common Adverse Reactions a in Two Placebo-Controlled Trials (1 and 2) in Adult Patients with IBS-C Adverse Reactions LINZESS 290 mcg [N=807] % Placebo [N=798] % Gastrointestinal Diarrhea Abdominal pain b Flatulence Abdominal distension 20 7 4 2 3 5 2 1 Infections and Infestations Viral Gastroenteritis 3 1 Nervous System Disorders Headache 4 3 a: Reported in at least 2% of LINZESS-treated patients and at an incidence greater than placebo b: “Abdominal pain” term includes abdominal pain, upper abdominal pain, and lower abdominal pain. Adverse reactions in an additional placebo-controlled trial in 614 IBS-C patients randomized to placebo or LINZESS 290 mcg once daily on an empty stomach for 12 weeks (Trial 6) were similar to those in Table 1. Diarrhea Diarrhea was the most commonly reported adverse reaction of the LINZESS-treated patients in the pooled IBS-C pivotal placebo-controlled trials. In these trials, 20% of LINZESS-treated patients reported diarrhea compared to 3% of placebo-treated patients. Severe diarrhea was reported in 2% of the LINZESS-treated patients versus less than 1% of the placebo-treated patients, and 5% of LINZESS-treated patients discontinued due to diarrhea vs less than 1% of placebo-treated patients. The majority of reported cases of diarrhea started within the first 2 weeks of LINZESS treatment [see Warnings and Precautions ( 5.2 )] . Adverse Reactions Leading to Discontinuation In placebo-controlled trials in patients with IBS-C, 9% of patients treated with LINZESS and 3% of patients treated with placebo discontinued prematurely due to adverse reactions. In the LINZESS-treatment group, the most common reasons for discontinuation due to adverse reactions were diarrhea (5%) and abdominal pain (1%). In comparison, less than 1% of patients in the placebo group withdrew due to diarrhea or abdominal pain. Adverse Reactions Leading to Dose Reductions In the open-label, long-term trials, 2147 patients with IBS-C received 290 mcg of LINZESS daily for up to 18 months. In these trials, 29% of patients had their dose reduced or suspended secondary to adverse reactions, the majority of which were diarrhea or other GI adverse reactions. Less Common Adverse Reactions Defecation urgency, fecal incontinence, vomiting, and gastroesophageal reflux disease were reported in <2% of patients in the LINZESS-treatment group and at an incidence greater than in the placebo treatment group. IBS- C in Pediatric Patients 7 Years of Age and Older The safety of LINZESS 145 mcg once daily was evaluated in 55 pediatric patients 7 to 17 years of age with IBS-C in a 12-week double-blind, parallel-group clinical trial (Trial 8) [see Clinical Studies ( 14.2 )] . The safety profile in pediatric patients treated with LINZESS was similar to the safety profile from trials in adults with IBS-C and CIC and in pediatric patients with FC. Diarrhea was the most common adverse reaction reported in 7% of 145 mcg LINZESS-treated pediatric patients. Most reported cases of diarrhea started within the first 2 weeks of LINZESS treatment [see Warnings and Precautions ( 5.2 )] . Chronic Idiopathic Constipation (CIC) in Adults Most Common Adverse Reactions The data described below reflect exposure to LINZESS in the two double-blind placebo-controlled clinical trials of 1275 adult patients with CIC (Trials 3 and 4) [see Clinical Studies ( 14.3 )] . Patients were randomized to receive placebo or 145 mcg LINZESS or 290 mcg LINZESS once daily on an empty stomach, for at least 12 weeks. Table 2 provides the incidence of adverse reactions reported in at least 2% of CIC patients in the 145 mcg LINZESS treatment group and at an incidence that was greater than in the placebo treatment group. Table 2: Most Common Adverse Reactions a in the Two Placebo-controlled Trials (3 and 4) in Adult Patients with CIC Adverse Reactions LINZESS 145 mcg [N=430] % Placebo [N=423] % Gastrointestinal Diarrhea Abdominal pain b Flatulence Abdominal distension 16 7 6 3 5 6 5 2 Infections and Infestations Upper respiratory tract infection Sinusitis 5 3 4 2 a: Reported in at least 2% of LINZESS-treated patients and at an incidence greater than placebo b: “Abdominal pain” term includes abdominal pain, upper abdominal pain, and lower abdominal pain. The safety of a 72 mcg dose was evaluated in an additional placebo-controlled trial in which 1223 patients were randomized to LINZESS 72 mcg, 145 mcg, or placebo once daily for 12 weeks (Trial 5). In Trial 5, adverse reactions that occurred at a frequency of ≥ 2% in LINZESS-treated patients (N=411 in each LINZESS 72 mcg and 145 mcg group) and at a higher rate than placebo (N=401) were: Diarrhea (LINZESS 72 mcg 19%; LINZESS 145 mcg 22%; placebo 7%) Abdominal distension (LINZESS 72 mcg 2%; LINZESS 145 mcg 1%; placebo < 1%) Diarrhea In Trials 3 and 4 (pooled) and Trial 5, diarrhea was the most commonly reported adverse reaction in LINZESS-treated patients in the CIC placebo-controlled studies. In all trials, the majority of reported cases of diarrhea started within the first 2 weeks of LINZESS treatment. Severe diarrhea was reported in less than 1% of the 72 mcg LINZESS-treated patients (Trial 5), in 2% of the 145 mcg LINZESS-treated patients (Trials 3, 4, and 5), and less than 1% of the placebo-treated patients (Trials 3, 4, and 5) [see Warnings and Precautions ( 5.2 )] . Adverse Reactions Leading to Discontinuation In placebo-controlled trials in patients with CIC, 3% of patients treated with 72 mcg (Trial 5) and between 5% and 8% (Trials 3, 4, and 5) of patients treated with 145 mcg of LINZESS discontinued prematurely due to adverse reactions compared to between less than 1% and 4% (Trials 3, 4, and 5) of patients treated with placebo. In patients treated with 72 mcg LINZESS, the most common reason for discontinuation due to adverse reactions was diarrhea (2% in Trial 5) and, in patients treated with 145 mcg LINZESS, the most common reasons for discontinuation due to adverse reactions were diarrhea (between 3% and 5% in Trials 3, 4, and 5) and abdominal pain (1% in Trials 3 and 4). In comparison, less than 1% of patients in the placebo group withdrew due to diarrhea or abdominal pain (Trials 3, 4, and 5). Adverse Reactions Leading to Dose Reductions In the open-label, long-term trials, 1129 patients with CIC received 290 mcg of LINZESS daily for up to 18 months. In these trials, 27% of patients had their dose reduced or suspended secondary to adverse reactions, the majority of which were diarrhea or o
Mechanism of action
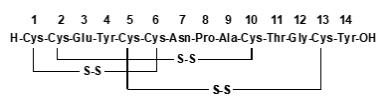
Mechanism of Action Linaclotide is structurally related to human guanylin and uroguanylin and functions as a guanylate cyclase-C (GC-C) agonist. Both linaclotide and its active metabolite bind to GC-C and act locally on the luminal surface of the intestinal epithelium. Activation of GC-C results in an increase in both intracellular and extracellular concentrations of cyclic guanosine monophosphate (cGMP). Elevation in intracellular cGMP stimulates secretion of chloride and bicarbonate into the intestinal lumen, mainly through activation of the cystic fibrosis transmembrane conductance regulator (CFTR) ion channel, resulting in increased intestinal fluid and accelerated transit. In animal models, linaclotide has been shown to both accelerate GI transit and reduce intestinal pain. In an animal model of visceral pain, linaclotide reduced abdominal muscle contraction and decreased the activity of pain-sensing nerves by increasing extracellular cGMP.
A drug lookup is just the start. Eleplan keeps the whole care plan in one place.
Medications, diagnoses, documents, appointments, and the whole care team — organized and always in sync, with Ellie, your AI care assistant, on top of it. Free to start.