24 HR amphetamine 15 MG Extended Release Oral Tablet — Centrally acting sympathomimetics. INDICATIONS AND USAGE Amphetamine sulfate tablets, USP 5 mg and 10 mg are indicated for: 1. Narcolepsy 2. Attention Deficit Disorder with Hyperactivit
Boxed warning
WARNING: ABUSE, MISUSE, AND ADDICTION Amphetamine extended-release orally disintegrating tablets have a high potential for abuse and misuse, which can lead to the development of a substance use disorder, including addiction. Misuse and abuse of CNS stimulants, including amphetamine extended-release orally disintegrating tablets, can result in overdose and death [see Overdosage ( 10) ] , and this risk is increased with higher doses or unapproved methods of administration, such as snorting or injection. Before prescribing amphetamine extended-release orally disintegrating tablets, assess each patient’s risk for abuse, misuse, and addiction. Educate patients and their families about these risks, proper storage of the drug, and proper disposal of any unused drug. Throughout amphetamine extended-release orally disintegrating tablets treatment, reassess each patient’s risk of abuse, misuse, and addiction and frequently monitor for signs and symptoms of abuse, misuse, and addiction [see Warnings and Precautions ( 5.1 ), Drug Abuse and Dependence ( 9.2 )] . WARNING: ABUSE, MISUSE AND ADDICTION See full prescribing information for complete boxed warning. Amphetamine extended-release orally disintegrating tablets have a high potential for abuse and misuse, which can lead to the development of a substance use disorder, including addiction. Misuse and abuse of CNS stimulants, including amphetamine extended-release orally disintegrating tablets, can result in overdose and death ( 5.1 , 9.2 , 10 ): Before prescribing amphetamine extended-release orally disintegrating tablets, assess each patient’s risk for abuse, misuse, and addiction. Educate patients and their families about these risks, proper storage of the drug, and proper disposal of any unused drug. Throughout treatment, reassess each patient’s risk and frequently monitor for signs and symptoms of abuse, misuse, and addiction.
majorpropoxyphene — potentiation of CNS stimulation and risk of convulsions
majorveratrum alkaloids — inhibition of hypotensive effect
Real-world adverse events (FAERS)
Drug Ineffective5,127Fatigue3,435Nausea3,078Headache2,878Anxiety2,667Depression2,243Toxicity to Various Agents2,232Feeling Abnormal2,117
Indications
INDICATIONS AND USAGE Amphetamine sulfate tablets, USP 5 mg and 10 mg are indicated for: 1. Narcolepsy 2. Attention Deficit Disorder with Hyperactivity as an integral part of a total treatment program which typically includes other remedial measures (psychological, educational, social) for a stabilizing effect in children with behavioral syndrome characterized by the following group of developmentally inappropriate symptoms: moderate to severe distractibility, short attention span, hyperactivity, emotional lability, and impulsivity. The diagnosis of the syndrome should not be made with finality when these symptoms are only of comparatively recent origin. Nonlocalizing (soft) neurological signs, learning disability, and abnormal EEG may or may not be present, and a diagnosis of central nervous system dysfunction may or not be warranted. 3. Exogenous Obesity as a short term (a few weeks) adjunct in a regimen of weight reduction based on caloric restriction for patients refractory to alternative therapy, e.g., repeated diets, group programs, and other drugs. The limited usefulness of amphetamines (see CLINICAL PHARMACOLOGY ) should be weighed against possible risks inherent in use of the drug, such as those described below.
Dosage
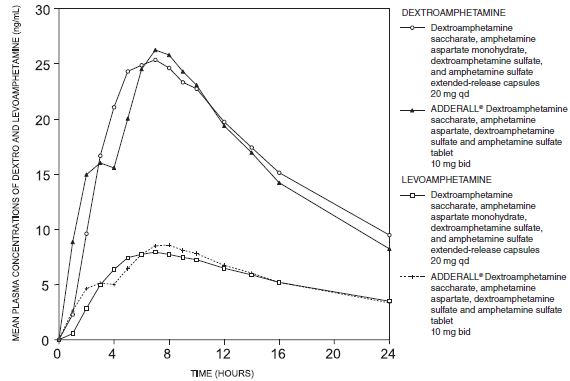
DOSAGE AND ADMINISTRATION May be taken with or without food. Allow tablet to disintegrate in saliva then swallow. ( 2.2 ) Pediatric patients (ages 6 to 17 years): Starting dose is 6.3 mg once daily in the morning. Maximum dose is 18.8 mg once daily for patients 6 to 12 years, and 12.5 mg once daily for patients 13 to 17 years. ( 2.3 ) Adults: 12.5 mg once daily in the morning. ( 2.4 ) To avoid substitution errors and overdosage, do not substitute for other amphetamine products on a milligram-per-milligram basis because of different amphetamine base compositions and differing pharmacokinetic profiles. ( 2.5 , 5.7 ) 2.1 Pre-treatment Screening Prior to treating patients with amphetamine extended-release orally disintegrating tablets, assess: for the presence of cardiac disease (i.e., perform a careful history, family history of sudden death or ventricular arrhythmia, and physical exam) [see Warnings and Precautions ( 5.2 ) ] . the family history and clinically evaluate patients for motor or verbal tics or Tourette’s syndrome before initiating amphetamine extended-release orally disintegrating tablets [see Warnings and Precautions ( 5.9 )] . 2.2 General Administration Information Amphetamine extended-release orally disintegrating tablets may be taken orally with or without food. Individualize the dosage according to the therapeutic needs and response of the patient. Amphetamine extended-release orally disintegrating tablets should be taken as follows: The tablet should remain in the blister pack until the patient is ready to take it. The patient or caregiver should use dry hands to open the blister. Tear along the perforation, bend the blister where indicated and peel back the blister’s labeled backing to take out the tablet. The tablet should not be pushed through the foil. As soon as the blister is opened, the tablet should be removed and placed on the patient’s tongue. The whole tablet should be placed on the tongue and allowed to disintegrate without chewing or crushing. The tablet will disintegrate in saliva so that it can be swallowed. 2.3 Dosage Recommendations in Pediatric Patients The recommended starting dosage is 6.3 mg once daily in the morning. Increase in increments of 3.1 mg or 6.3 mg at weekly intervals. The maximum recommended dose is 18.8 mg daily for patients 6 to 12 years, and 12.5 mg daily for patients 13 to 17 years [see Use in Specific Populations ( 8.3 ) , Clinical Studies ( 14 ) ] . 2.4 Dosage Recommendations in Adults The recommended dose is amphetamine extended-release orally disintegrating tablets 12.5 mg daily. 2.5 Switching from Other Amphetamine Products Patients taking dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine aspartate monohydrate, and amphetamine sulfate extended-release capsules may be switched to amphetamine extended-release orally disintegrating tablets at the equivalent dose taken once daily [see Clinical Pharmacology ( 12.3 )] . Refer to Table 1 for equivalent doses of amphetamine extended-release orally disintegrating tablets and dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine aspartate monohydrate, and amphetamine sulfate extended-release capsules. Dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine aspartate monohydrate, and amphetamine sulfate extended-release capsules are also referred to as mixed salts of a single-entity amphetamine product extended-release capsules (MAS ER). Table 1: Equivalent Doses of Amphetamine Extended-Release Orally Disintegrating Tablets and Dextroamphetamine Sulfate, Dextroamphetamine Saccharate, Amphetamine Aspartate Monohydrate, and Amphetamine Sulfate (Mixed Salts of a Single-Entity Amphetamine Product) Extended-Release Capsules Amphetamine extended-release orally disintegrating tablets 3.1 mg 6.3 mg 9.4 mg 12.5 mg 15.7 mg 18.8 mg Dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine aspartate monohydrate, and amphetamine sulfate extended-release capsules Mixed salts of a single-entity amphetamine product extended-release capsules (MAS ER) 5 mg 10 mg 15 mg 20 mg 25 mg 30 mg If switching from any other amphetamine products, discontinue that treatment, and titrate with amphetamine extended-release orally disintegrating tablets using the titration schedule [see Dosage and Administration ( 2.3 ) , ( 2.4 ) ] . Do not substitute for other amphetamine products on a milligram-per-milligram basis because of different amphetamine base compositions and differing pharmacokinetic profiles [see Warnings and Precautions ( 5.9 )] . 2.6 Dosage Modifications Due to Drug Interactions Agents that alter urinary pH can impact urinary excretion and alter blood levels of amphetamine. Acidifying agents (e.g., ascorbic acid) decrease blood levels, while alkalinizing agents (e.g., sodium bicarbonate) increase blood levels. Adjust amphetamine extended-release orally disintegrating tablets dosage accordingly [see Drug Interactions ( 7.1 )] .
Warnings
WARNING Serious Cardiovascular Events Sudden Death and Pre-Existing Structural Cardiac Abnormalities or Other Serious Heart Problems Children and Adolescents Sudden death has been reported in association with CNS stimulant treatment at usual doses in children and adolescents with structural cardiac abnormalities or other serious heart problems. Although some serious heart problems alone carry an increased risk of sudden death, stimulant products generally should not be used in children or adolescents with known serious structural cardiac abnormalities, cardiomyopathy, serious heart rhythm abnormalities, or other serious cardiac problems that may place them at increased vulnerability to the sympathomimetic effects of a stimulant drug (see CONTRAINDICATIONS ). Adults Sudden deaths, stroke, and myocardial infarction have been reported in adults taking stimulant drugs at usual doses for ADHD. Although the role of stimulants in these adult cases is also unknown, adults have a greater likelihood than children of having serious structural cardiac abnormalities, cardiomyopathy, serious heart rhythm abnormalities, coronary artery disease, or other serious cardiac problems. Adults with such abnormalities should also generally not be treated with stimulant drugs (see CONTRAINDICATIONS ). Hypertension and other Cardiovascular Conditions Stimulant medications cause a modest increase in average blood pressure (about 2 to 4 mmHg) and average heart rate (about 3 to 6 bpm), and individuals may have larger increases. While the mean changes alone would not be expected to have short-term consequences, all patients should be monitored for larger changes in heart rate and blood pressure. Caution is indicated in treating patients whose underlying medical conditions might be compromised by increases in blood pressure or heart rate, e.g., those with pre-existing hypertension, heart failure, recent myocardial infarction, or ventricular arrhythmia (see CONTRAINDICATIONS ). Assessing Cardiovascular Status in Patients being Treated with Stimulant Medications Children, adolescents, or adults who are being considered for treatment with stimulant medications should have a careful history (including assessment for a family history of sudden death or ventricular arrhythmia) and physical exam to assess for the presence of cardiac disease, and should receive further cardiac evaluation if findings suggest such disease (e.g., electrocardiogram and echocardiogram). Patients who develop symptoms such as exertional chest pain, unexplained syncope, or other symptoms suggestive of cardiac disease during stimulant treatment should undergo a prompt cardiac evaluation. Psychiatric Adverse Events Pre-Existing Psychosis Administration of stimulants may exacerbate symptoms of behavior disturbance and thought disorder in patients with a pre-existing psychotic disorder. Bipolar Illness Particular care should be taken in using stimulants to treat ADHD in patients with comorbid bipolar disorder because of concern for possible induction of a mixed/manic episode in such patients. Prior to initiating treatment with a stimulant, patients with comorbid depressive symptoms should be adequately screened to determine if they are at risk for bipolar disorder; such screening should include a detailed psychiatric history, including a family history of suicide, bipolar disorder, and depression. Emergence of New Psychotic or Manic Symptoms Treatment emergent psychotic or manic symptoms, e.g., hallucinations, delusional thinking, or mania in children and adolescents without a prior history of psychotic illness or mania can be caused by stimulants at usual doses. If such symptoms occur, consideration should be given to a possible causal role of the stimulant, and discontinuation of treatment may be appropriate. In a pooled analysis of multiple short-term, placebo-controlled studies, such symptoms occurred in about 0.1% (4 patients with events out of 3482 exposed to methylphenidate or amphetamine for several weeks at usual doses) of stimulant-treated patients compared to 0 in placebo-treated patients. Aggression Aggressive behavior or hostility is often observed in children and adolescents with ADHD, and has been reported in clinical trials and the postmarketing experience of some medications indicated for the treatment of ADHD. Although there is no systematic evidence that stimulants cause aggressive behavior or hostility, patients beginning treatment for ADHD should be monitored for the appearance of or worsening of aggressive behavior or hostility. Long-Term Suppression of Growth Careful follow-up of weight and height in children ages 7 to 10 years who were randomized to either methylphenidate or non-medication treatment groups over 14 months, as well as in naturalistic subgroups of newly methylphenidate-treated and non-medication treated children over 36 months (to the ages of 10 to 13 years), suggests that consistently medicated children (i.e., treatment for 7 days per week throughout the year) have a temporary slowing in growth rate (on average, a total of about 2 cm less growth in height and 2.7 kg less growth in weight over 3 years), without evidence of growth rebound during this period of development. Published data are inadequate to determine whether chronic use of amphetamines may cause a similar suppression of growth, however, it is anticipated that they likely have this effect as well. Therefore, growth should be monitored during treatment with stimulants, and patients who are not growing or gaining height or weight as expected may need to have their treatment interrupted. Seizures There is some clinical evidence that stimulants may lower the convulsive threshold in patients with prior history of seizures, in patients with prior EEG abnormalities in absence of seizures, and, very rarely, in patients without a history of seizures and no prior EEG evidence of seizures. In the presence of seizures, the drug should be discontinued. Peripheral Vasculopathy, including Raynaud's phenomenon Stimulants, including Amphetamine Sulfate Tablets, used to treat ADHD are associated with peripheral vasculopathy, including Raynaud's phenomenon. Signs and symptoms are usually intermittent and mild; however, very rare sequelae include digital ulceration and/or soft tissue breakdown. Effects of peripheral vasculopathy, including Raynaud's phenomenon, were observed in post-marketing reports at different times and at therapeutic doses in all age groups throughout the course of treatment. Signs and symptoms generally improve after reduction in dose or discontinuation of drug. Careful observation for digital changes is necessary during treatment with ADHD stimulants. Further clinical evaluation (e.g., rheumatology referral) may be appropriate for certain patients. Serotonin Syndrome Serotonin syndrome, a potentially life-threatening reaction, may occur when amphetamines are used in combination with other drugs that affect the serotonergic neurotransmitter systems such as monoamine oxidase inhibitors (MAOIs), selective serotonin reuptake inhibitors (SSRIs), serotonin norepinephrine reuptake inhibitors (SNRIs), triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, tryptophan, buspirone, and St. John's Wort (see DRUG INTERACTIONS ). Amphetamines and amphetamine derivatives are known to be metabolized, to some degree, by cytochrome P450 2D6 (CYP2D6) and display minor inhibition of CYP2D6 metabolism (see CLINICAL PHARMACOLOGY ). The potential for a pharmacokinetic interaction exists with the co-administration of CYP2D6 inhibitors which may increase the risk with increased exposure to Amphetamine Sulfate Tablets. In these situations, consider an alternative non-serotonergic drug or an alternative drug that does not inhibit CYP2D6 (see DRUG INTERACTIONS ). Serotonin syndrome symptoms may include mental status changes (e.g., agitation, hallucinations, delirium, and coma), autonomic instability (e.g., tachycardia, labile blo
Contraindications
CONTRAINDICATIONS Amphetamine extended-release orally disintegrating tablets are contraindicated: In patients known to be hypersensitive to amphetamine, or other components of amphetamine extended-release orally disintegrating tablets. Hypersensitivity reactions such as angioedema and anaphylactic reactions have been reported in patients treated with other amphetamine products [see Adverse Reactions ( 6.2 )] . Patients taking monoamine oxidase inhibitors (MAOIs), or within 14 days of stopping MAOIs (including MAOIs such as linezolid or intravenous methylene blue), because of an increased risk of hypertensive crisis [see Warnings and Precautions ( 5.7 ), Drug Interactions ( 7.1 )] . Known hypersensitivity to amphetamine products or other ingredients in amphetamine extended-release orally disintegrating tablets. ( 4 ) Use of monoamine oxidase inhibitor (MAOI) or within 14 days of the last MAOI dose. ( 4 )
Mechanism of action
CLINICAL PHARMACOLOGY Amphetamines are non-catecholamine, sympathomimetic amines with CNS stimulant activity. Peripheral actions include elevations of systolic and diastolic blood pressures, and weak bronchodilator, and respiratory stimulant action. Amphetamine, as the racemic form, differs from dextroamphetamine in a number of ways. The l-isomer is more potent than the d-isomer in cardiovascular activity, but much less potent in causing CNS excitatory effects. The racemic mixture also is less effective as an appetite suppressant when compared to dextroamphetamine. There is neither specific evidence which clearly establishes the mechanism whereby amphetamines produce mental and behavioral effects in children, nor conclusive evidence regarding how those effects relate to the condition of the central nervous system. Drugs in this class used in obesity are commonly known as "anorectics" or "anorexigenics." It has not been established, however, that the action of such drugs in treating obesity is primarily one of appetite suppression. Other central nervous system actions or metabolic effects, may be involved, for example. Adult obese subjects instructed in dietary management and treated with "anorectic" drugs lose more weight on the average than these treated with placebo and diet, as determined in relatively short- term clinical trials. The magnitude of increased weight loss of drug-treated patients over placebo-treated patients is only a fraction of a pound a week. The rate of weight loss is greatest in the first weeks of therapy for both drug and placebo subjects and tends to decrease in succeeding weeks. The origins of the increased weight loss due to the various possible drug effects are not established. The amount of weight loss associated with the use of an "anorectic" drug varies from trial to trial, and the increased weight loss appears to be related in part to variables other than the drug prescribed, such as the physician-investigator, the population treated, and the diet prescribed. Studies do not permit conclusions as to the relative importance of the drug and nondrug factors on weight loss. The natural history of obesity is measured in years, whereas the studies cited are restricted to few weeks duration; thus, the total impact of drug-induced weight loss over that of diet alone must be considered clinically limited.
A drug lookup is just the start. Eleplan keeps the whole care plan in one place.
Medications, diagnoses, documents, appointments, and the whole care team — organized and always in sync, with Ellie, your AI care assistant, on top of it. Free to start.